Zambia: One grim example of how Trump has slashed anti-AIDS efforts
Zambia’s anti-HIV program, which saved 100,000s of lives, has begun to crumble.
Dire predictions immediately followed the Trump administration’s decision in early 2025 to impose drastic cuts on foreign aid in general and the President’s Emergency Plan for AIDS Relief (Pepfar) in particular.
The Lancet medical journal forecast that Trump administration cuts in USAID funding “would result in approximately 1,776,539 all-age deaths and 689,900 deaths in children younger than 5 years” in 2025 alone.
Over the coming five years, the Lancet said, “the complete defunding of U.S.A.I.D. would cause an estimated 2,450,000 all-age deaths annually, leading to a total of 14,051,750 excess all-age deaths and 4,537,157 excess under-5 deaths by 2030.”
In fact, many such deaths have occurred, though the magnitude of the disaster is hard to see since it is spread across dozens of nations where news coverage is sparse. The disaster may fall short of the Lancet’s forecast, but it remains a tragedy.
That is apparent in individual nations that depended on US support for anti-AIDS efforts. For example, The New York Times has taken a close look at what is happening in Zambia.
The Times reporter who wrote the Zambia article commented on what she found:
I first reported on H.I.V. in Zambia in 2002, when treatment was nearly impossible to find across sub-Saharan Africa. I saw villages where grandmothers raised dozens of orphans and hospital wards where gaunt, dying patients packed the corridors. Over the next few years, it was astonishing to see Zambia — bolstered by international donors and the U.S. PEPFAR program — turn the tide. More than a million people gained access to medication, and H.I.V. became a manageable chronic condition.


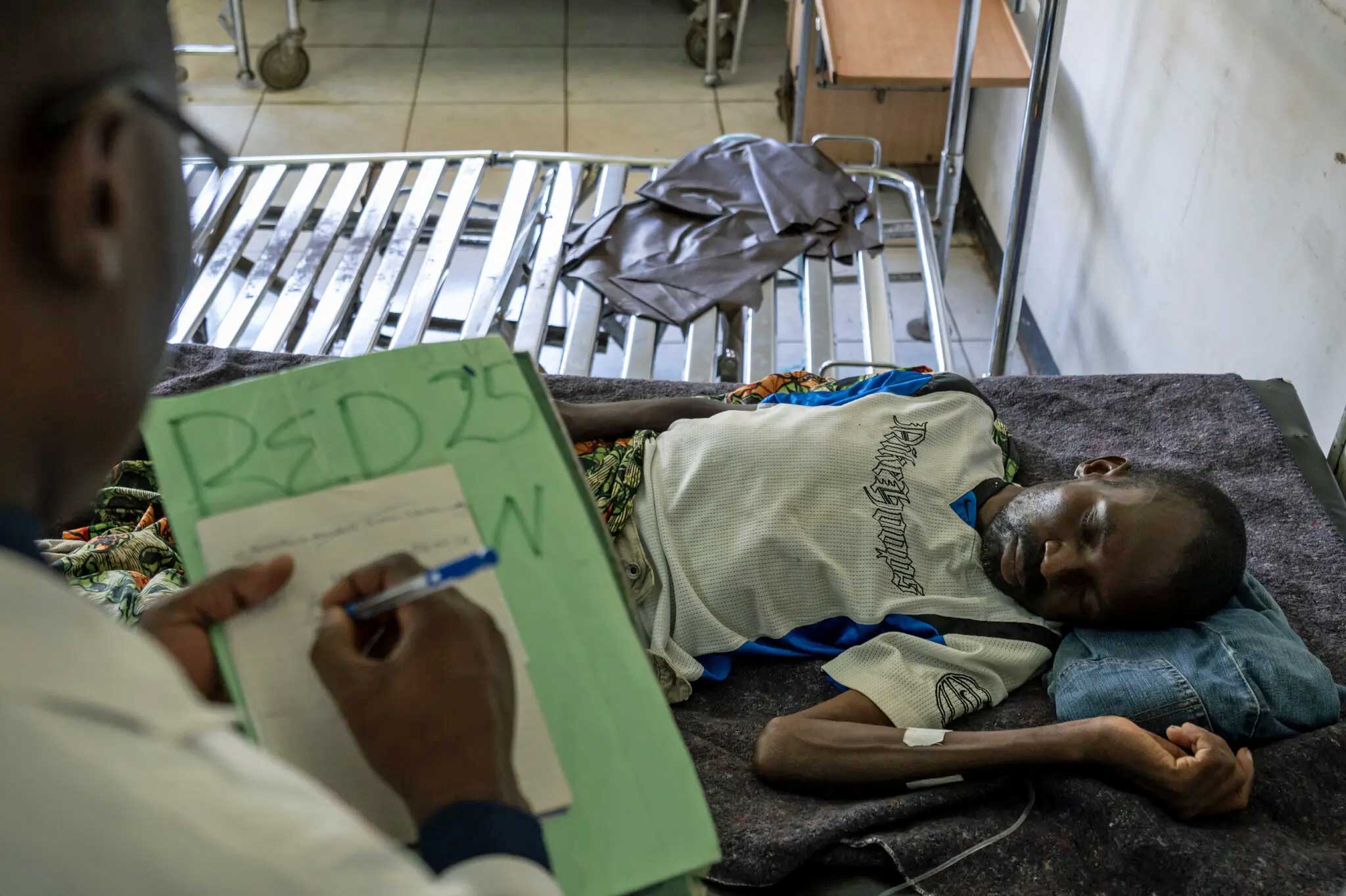
That is why it took my breath away to walk into a northern mission hospital recently and see men clearly dying of AIDS. While Zambia has managed to keep its core H.I.V. program running despite drastically reduced U.S. support, the cracks are widening. In clinics across the country, the human toll of this funding gap is becoming painfully visible.
One reader commented further:
As someone whose uncle died of AIDS when I was 16 in 1992, and I remember that many in the community were dying as well, this is predictable and at the same time a demonstration of how heartless and shameful the United States has been in cutting funding for AIDS. It shows how ignorant of history the Trump administration has been, as if the United States wants to add more deaths to the AIDS epidemic in the Western countries and Africa.
What AIDS does is to destroy an entire community by destroying families, parents, partners, elders, leaders, youth. Should USAID have been helping these countries become less dependent on aid? Of course. But this is quite impossible in the short term as the medicine comes from the western world and the infrastructure for delivering this medicine is dependent on a stable government structure, which most developing countries do not have. And we are complacently looking the other way while hundreds of thousands of people die. The United States is a frightening country, we proclaim our greatness but hoard basic necessities of life, for meaningless reasons.
Excerpts from the New York Times article are below;
AIDS Creeps Back in Parts of Zambia, a Year After U.S. Cuts to H.I.V. Assistance
A once-robust H.I.V. treatment and prevention system, credited with saving hundreds of thousands of lives, has begun to crumble.
Saulo Kasekela died of AIDS on March 7, in a small town called Mpongwe in the copper belt of northern Zambia. He was a 37-year-old security guard, admitted to the mission hospital two days earlier. After his body was wheeled out of the men’s ward, a nurse set aside his chest X-ray, a clouded smear of lungs devoured by tuberculosis, a hallmark of advanced, untreated H.I.V. infection. A scrawled doctor’s note indicated the X-ray should be saved for medical students.
Of the eight patients in the ward that day, four had AIDS. Lewis Chifuta, 33, was bone thin, feverish and barely able to recognize his siblings when they reached his bedside.
A year ago, in Mpongwe, there was one case like this each month, or maybe two. In January this year, there were 28 new cases; in February, 28 more; in March, seven more.
During President Trump’s first month in office, his administration upended much of the flagship global H.I.V. program that had saved the lives of hundreds of thousands of people in Zambia. The Zambian government went into emergency mode, desperate to ensure that people with the virus could continue to receive lifesaving medications.
But other crucial aspects of the program had to be scrapped — interventions that had helped stop the spread of the virus and protected the most vulnerable people, those like Mr. Kasekela.
Today, a pared-down system is operating on reduced U.S. support, and Zambia may lose that help entirely in the next few days. The Trump administration has set an April 30 deadline for the Zambian government to accept a new health funding agreement that is tied to giving the United States expanded access to the country’s mineral resources.
The administration says the deal would offer Zambia five years of funding and help to build a stronger system that gives the country more control. But if Zambia doesn’t sign, officials warn that Washington could cut off all of its H.I.V. aid, a situation health officials here say would be disastrous.
What is happening in Mpongwe now is a grim echo of a time that most of the nurses and clinicians here are not old enough to remember. Three decades ago, hospitals in Zambia were packed with young men and women dying agonizing deaths, and the H.I.V./AIDS pandemic had overwhelmed the health system. Life expectancy had dropped to 37.
In 2003, President George W. Bush’s administration launched a historic humanitarian response to the pandemic — the President’s Emergency Plan for AIDS Relief, or PEPFAR — and Zambia was a focus country. By then, a lifesaving cocktail of antiretroviral medications had beaten back AIDS in the United States and other high-income countries, but the drugs cost tens of thousands of dollars, and almost no one in Africa could get them.
PEPFAR changed all that. Hundreds of thousands of people were given free access to those drugs in cheap generic forms. The United States built a network of laboratories and clinics that drew on the best of American innovation and technology. The rate of new infections was driven steadily down. Life expectancy in Zambia rose back to 67.
Then, last year, as part of its restructuring of foreign aid, the Trump administration cut off its funding for H.I.V. programs, saying many of the programs had been wasteful and an inappropriate use of taxpayer dollars.
Then it restored some of the funding, then withheld some. The United States Agency for International Development was delivering PEPFAR services in the northern half of Zambia — the region with highest rates of H.I.V. prevalence and transmission in the country — through dozens of local organizations. They closed abruptly.
Zambia’s top officials held emergency meetings and sent a directive to provincial health offices: Redeploy whatever staff you have to keep the antiretroviral medication moving.
“It was like a military state of emergency,” said Dr. Suilanji Sivile, the national technical adviser to the H.I.V. program. They managed it: 2,885 treatment facilities, a vast majority, have stayed open, he said. Most of the medications they distribute were purchased by the United States.
Today, the Zambian government says that most of the 1.3 million people who were on H.I.V. treatment in January 2025 are still receiving their drugs. (The health ministry estimates that 100,000 people stopped taking their medication in the upheaval, and 40,000 of them have yet to be re-engaged.)
But because many prevention services have been cut, health officials fear infection rates are inevitably rising. Testing has been cut, too, though, so they cannot be sure how much or how quickly. Many new H.I.V. infections will not be caught until people are seriously ill, and by then they may have infected others.
Dr. Lloyd Mulenga, who leads Zambia’s national H.I.V. program, sat with his colleagues in early 2025 and did the painful exercise of deciding what services they would cut.
They kept the bare essentials, Dr. Mulenga said, but much else had to go:
When a person tested positive for H.I.V., a team traced that person’s sexual contacts, counseled and tested each of them and put them on H.I.V. treatment if they were infected. This labor-intensive system, known as index testing, found 70 percent of the infections identified each year. It has shut down.
Pregnant women with H.I.V. had the amount of virus in their system tested three times over their pregnancy, so that a clinician could respond quickly to any hint that their medication was failing and their fetus exposed. That testing has been cut to once.
Eswatini’s top court demands official recognition of LGBT advocacy group
Babies born to H.I.V.-positive mothers were tested for the virus through a highly accurate but expensive genetic test within hours of birth, and antiretroviral treatment was started immediately for those who tested positive. Now babies are not tested until 6 weeks old, when a cheaper standard blood test can be used.
Everyone who came to a medical center for any kind of care was tested for H.I.V. Now testing is restricted to people who ask for a test or who have another sexually transmitted infection or tuberculosis symptoms.
The genetics of the virus infecting people newly diagnosed were sequenced, indicating how new the infection was: When the data showed a number of recent infections in people from one place — like a hub on a trucking route, for example — a “hot zone” team could blanket the area with testing and prevention services. The ministry of health decided it could not fund that testing.
Antiretroviral drugs were distributed in communities — in small market shops, at churches — making it easy and discreet for people to get their medication. Those sites were closed.
Community health workers phoned people to remind them of appointments and, if they did not turn up, went to their homes or traced them to new locations, to make sure they did not miss a dose of medication. Most of those workers have lost their jobs.
People from communities that are highly vulnerable to H.I.V. infection but who may face harassment or shame in the main medical system — gay men, sex workers — received services in small, dedicated sites. Those have been closed.
At every H.I.V. treatment site, data teams used electronic records to track who was positive, who picked up their medications and whose viral load was uncontrolled — so that clinicians could track patients. Most have returned to using paper.
Teenage girls have for years been the demographic most likely to be infected with H.I.V. Dedicated programs worked to target them with H.I.V. prevention and educational and vocational training to motivate them to avoid infection. Those were closed.
More than 100,000 Zambian men were given free circumcisions each year. (Circumcised men are less likely to become infected or transmit H.I.V.) That program was canceled.
A year later, the impact of all these cuts is visible in the hospital wards and H.I.V. clinics in the copper belt.
At the mission hospital in Mpongwe, Dexter Fundulu, an H.I.V. clinician, closed out Mr. Kasekela’s file after he died. Mr. Fundulu had diagnosed Mr. Kasekela with H.I.V. in December. But his new patient lived about 40 miles from the hospital, and he did not show up to pick up his medications in January or February. The mobile community team that used to deliver medicines to patients like him had been eliminated.
It seemed, Mr. Fundulu said, that more patients had been missed, or fallen away from care, in the upheaval a year ago. Now the devastating symptoms of uncontrolled H.I.V. are catching up with them.
At a clinic in a gritty neighborhood called Chipulukusu, in the regional hub of Ndola, Maureen Dhaka, who has H.I.V., gave birth on March 5. The baby was chalky and silent, the umbilical cord wrapped around his neck, and an ambulance was summoned to take mother and infant to the children’s hospital.
There, the baby was placed on oxygen, and began to regain color. But no one tested him for H.I.V., even though his mother lives with the virus. No one gave him H.I.V. prophylaxis for nearly two full days after his birth, even though every moment counts to prevent an infection.
Before the cuts, a community health worker would have accompanied Ms. Dhaka and the baby to the hospital, and made sure the baby was swiftly given prophylaxis. Today, only one community health worker works at the Chipulukusu clinic, not five, and she did not catch up with Ms. Dhaka for days.
In Ipusukilo, a scrappy community outside the mining town of Kitwe, a 25-year-old patient named Precious Mulenga came to the H.I.V. clinic to pick up medication in February. When she arrived, she learned that the clinic — where a staff of 11 was reduced to just one for months after the funding cuts — had lost track of the results of a blood test she had taken last July. Those results were alarming: Her viral load was high. But there were no community health workers left to track her down to let her know, and help her take the correct medication to control it.